

Graft failure occurs in 3-5% of hematopoietic stem cell transplantations (HSCT) and raises up to 10% for mismatched HSCT. It is a severe complication leading to lethal infections or bleedings. Several studies reported that engraftment could be improved by mesenchymal stromal cells (MSCs) infusion. Those cells are multipotent cells capable of differentiation in at least 3 lineages (adipocytes, chondrocytes and osteocytes) and of supportive effects on hematopoiesis.
This treatment is considered as an Advanced Therapy Medicinal Product in France and there is currently no authorization for its use outside of clinical trials. We retrospectively analyzed the demands from HSCT French centers to the expert committee of the SFGMTC and the French regulatory agency (ANSM), since 2014, in order to ask for MSCs exceptional recourse for patients with graft failure.
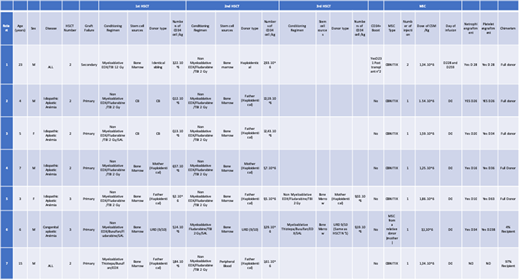
Nine requests for MSCs were made. One patient did not receive any MSCs because MSCs bag was contaminated, another one had an haploidentical transplantation without MSCs instead. Finally, 7 patients received 1 or 2 infusions of MSCs (Table).
Median age was of 6 years (4-23), sex ratio was of 2,5. Two patients (29%) had an acute lymphoblastic leukemia (ALL) and 5 patients (71%) had an aplastic anemia (idiopathic n=4, congenital n=1). Five patients had received one transplantation, and 2 patients had received two transplantations, followed by a primary graft failure (n=6) and a secondary graft failure (n=1). Only 2 patients had received a myeloablative conditioning regimen (MAC) for the first procedure, one chemo- and one TBI- based. The other 5 patients had received a reduced-intensity conditioning (RIC) regimen, 4 of them with 2 grays TBI. Two patients had received a cord blood unit and 5 bone marrows from 1 sibling, 3 haploidentical and 1 mismatched donors. Only 2 patients had received antithymoglobulins in their previous regimen. Engraftments failed despite a median richness of 5,14.106 CD34 cells/kg/bone marrow graft (1,84-9,5) and of 1,25.105CD34 cells/kg/cord blood unit (1,2-1,3).
Median delay between first HSCT with graft failure and MSCs infusion was of 2 months (1-32). To prepare last HSCT,six patients received a reduced intensity conditioning regimen with 2 grays TBI (Baltimore), and one patient received a myeloablative, chemo-based, regimen, with antithymoglobulins. Three patients received a graft from the same previous donor. Six patients received a haploidentical graft (5 bone marrows, 1 peripheral blood stem cells), and 1 received bone marrow from a mismatched donor. Median number of CD34+ cells was of 9,02.106/kg (1,61-12,43).
All MSCs were from 8 pooled donors (OBNITIX®) except for one patient who received MSCs from a relative donor (which was different from the HSCT donor). All infusions were well tolerated and made on the same day as HSCT, apart from one patient who received MSCs for a secondary graft failure on day 228 post-transplantation, followed by an infusion of CD34+ cells on day 231, and a second infusion of MSCs on day 259. Mean dose of MSCs was of 1,72.106/kg (1,25-3,1).
Median time for neutrophil recovery (neutrophils over 0.5 G/L) and platelet recovery (platelets over 50 G/L) on 3 consecutive days was respectively of 23 days (10-34) and 35 days (26-238). At day 30, 5 patients (71%) had a full donor chimerism. Only one patient presented a graft failure leading to a third HSCT. No secondary graft failure occurred after a median follow-up of 13 months (4-104). At last follow-up, none of the patients who achieved platelet and neutrophil recovery required neither blood or platelets transfusion nor thrombopoietin receptor analogs. Infusion of MSCs at the time of HSCT to prevent graft failure was safe and effective for 6/7 patients. Larger prospective trials are necessary to confirm MSCs impact on engraftment and graft function.
Dalle:AbbVie Pharmacyclics: Membership on an entity's Board of Directors or advisory committees; Gilead: Honoraria; Jazz Pharmaceuticals: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Orchard: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Medac: Consultancy, Honoraria; Bellicum: Consultancy, Honoraria; Sanofi-Genzyme: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Novartis: Honoraria, Membership on an entity's Board of Directors or advisory committees; bluebird bio: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Incyte: Consultancy, Membership on an entity's Board of Directors or advisory committees. Rubio:Medac: Consultancy; Gilead: Honoraria; MSD: Honoraria; Novartis: Honoraria; Neovii: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal